
|
|
The issue of large goiters - case 765
|
|





Clinical presentation: A 41-year-old man was referred for aspiration cytology. First, he was examined for nodular goiter 9 years ago when FNA resulted in benign colloid goiter from a nodule with a 21-mm maximal diameter. Recently, cytology was repeated because the nodule has been grown to 42 mm. This time FNA was non-diagnostic.
Palpation: a not firm nodule in the right lobe.
Hormonal examination: TSH 1.47 mIU/L.
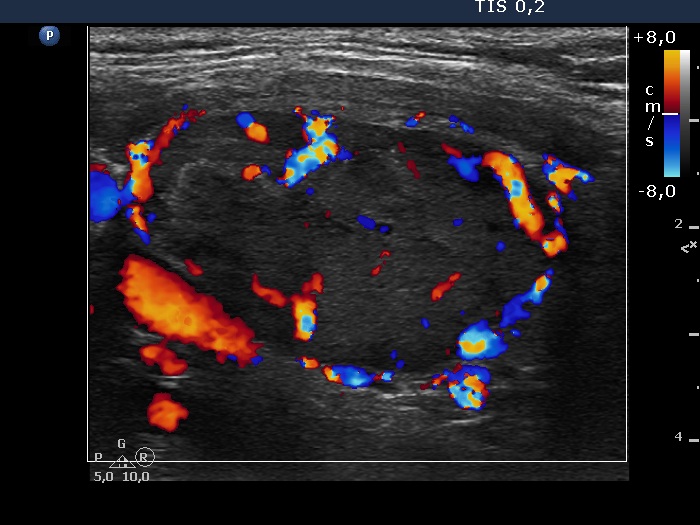
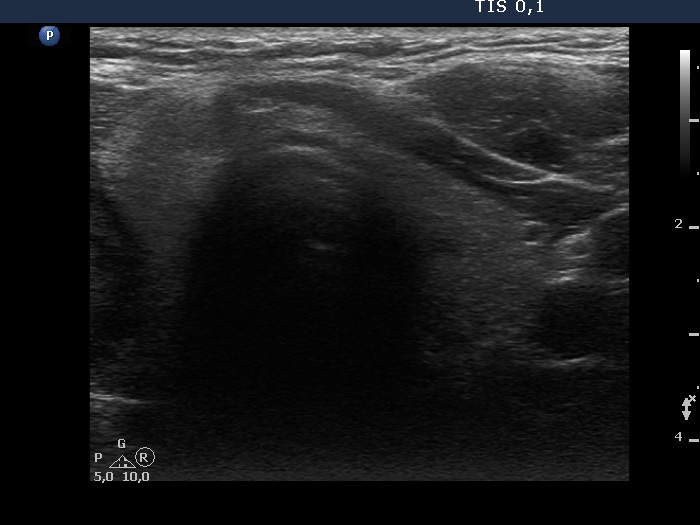
Ultrasonography. The thyroid was echonormal. There was a hypoechoic nodule in the right lobe. The dimensions of the nodule were 39x21x42 mm, width, depth and length, respectively. The lesion had a partial halo and both perinodular and intranodular vascularity.
Cytology was performed form the nodule. The pattern corresponded to a benign lesion: follicular cells were found in several regular sheets and dissociated. They displayed no significant atypia.
Considering the ultrasound presentation, we gave a combined sono-cytological diagnosis of suspicion of follicular tumor.
A right lobectomy was advised.
Histopathology in progress.
Comments.
-
On the ultrasound presentation, the likelihood of follicular tumor is around 90%.
-
We should always bear in mind, that cytology is not able to represent fully a nodule. A follicular tumor always has parts which architecture can correspond to a non-tumorous lesion and vice versa, microfollicles are integral parts of all thyroid pathologies and even of a normal thyroid. A cytological diagnosis of follicular tumor is based on the proportion of microfollicular structures. Considering the above-mentioned facts, cytological diagnosis of follicular tumor involves greater uncertainty than, for example, in the case of a papillary cancer.
-
In a large solitary nodule presenting either halo or perinodular vascularity, the likelihood of a follicular tumor is greater than 90%.
-
I will extend the case study when the histopathological diagnosis will be available.