
|
|
Thyroid cancers - case 1066
|
|











Clinical data: A 75-year-old man was referred for evaluation of a suddenly developed mass in the region of the left lobe. The tumor developed within 2 months. The patient has been operated on bladder cancer for 8 years, no recurrence was found on the last check 5 months ago.
We met the patient 8 years ago. The thyroid was echonormal. The right lobe had a solitary hypoechoic nodule with the dimensions of 12x10x13 mm, width, depth, length, respectively. FAN resulted in benign, colloid goiter.
Palpation: There was a large, very firm mass in the region of the left lobe and lateral to it.
Functional state: TSH 0.96 mIU/L.
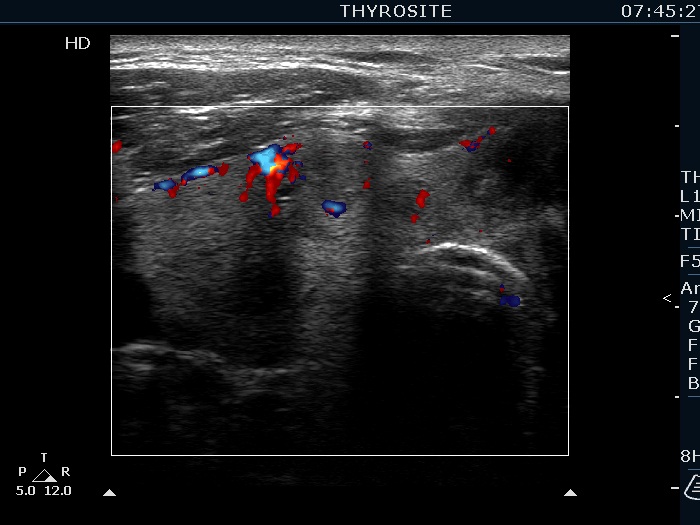
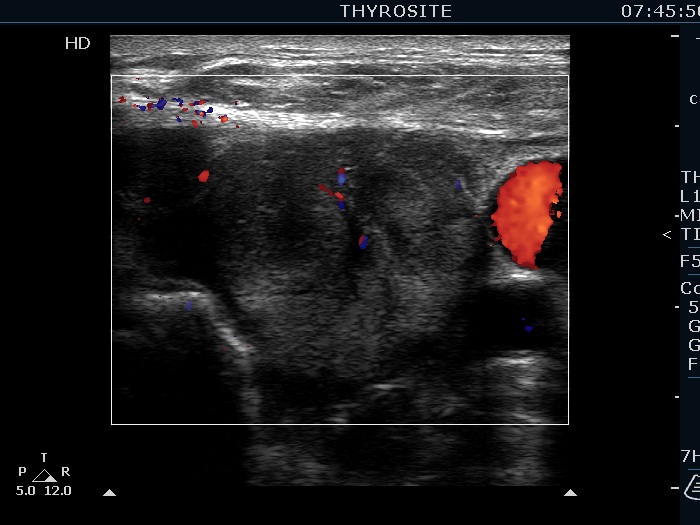
Ultrasonography. The right lobe was echonormal and presented several hypoechoic nodules. A large, inhomogeneous, partly deeply hypoechoic, partly minimally hypoechoic or echonormal mass occupied the left lobe. The borders of the tumor were irregular. There were multiple lymph nodules upper and lateral to the left thyroid lobe. The nodes had a heterogeneous pattern and lacked hilum. The vascularity was scanty both in the thyroid nodules and the lymph nodes.
Cytology resulted in not well differentiated cancer, probably metastasis of the bladder cancer.
Wash-out thyroglobulin determination was technically unsuccessful. We suggested a repeat test but the patient's relatives turned to the urologist who had previously treated him. We did not meet the patient again.
Surgery was performed more than 3 months after the cytological examination. During this period, the patient had numerous examinations including 7 CT scans and liver biopsy. Thyroid FNA was repeated twice in other institute, both resulted in metastasis. Histopathology disclosed anaplastic thyroid cancer.
Comments.
-
In our practice around 5% of wash-out determination are technically unsuccessful, i.e. the laboratory refuses the present data. In all but one of such cases, the repeat test was measurable. Had the patient come to repeat the wash-out, it would most likely have saved a lot of unnecessary testing.
-
The cytological pattern of anaplastic cancer of any origins is essentially the same. In this patient, both the clinical and the ultrasound appearance were misleading. The tumor developed significantly more slowly than usual and neck metastases were also present. These two things are, of course, related. Due to the high degree of aggression characteristic of anaplastic cancer, it is much more common to see direct spread and there is no time to develop metastases.