
|
|
Thyroid cancers - case 1270
|
|








Clinical data: A 57-year-old man was referred for evaluation of a rapidly increasing mass in the left side of the neck. He first noticed the lump for 4 months.
Palpation: a very hard mass involving the left lobe and the left side of the neck. The mass was around 12 cm in maximal diameter.
Functional state: euthyroidism (TSH 3.41 mIU/L).
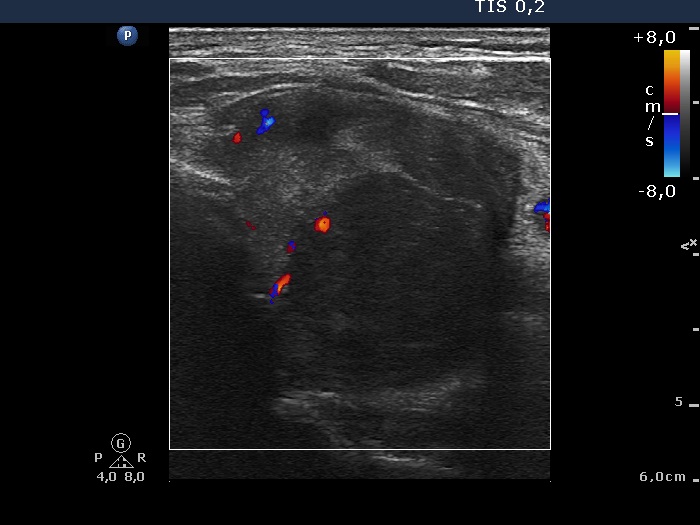
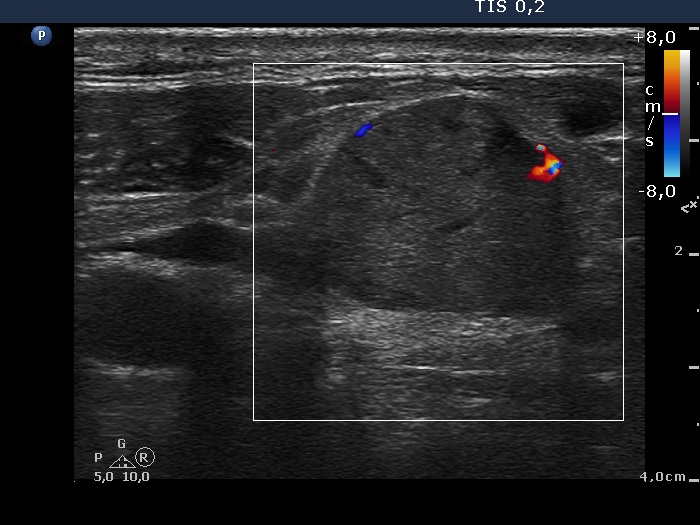
Ultrasonography revealed that the palpable mass contained the enlarged left thyroid composed of a large hypoechogenic nodule with irregular borders and multiple irregular lymph nodes in the left side of the neck.
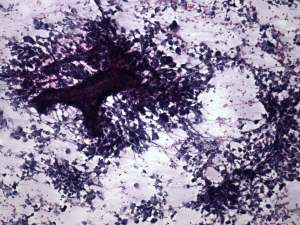
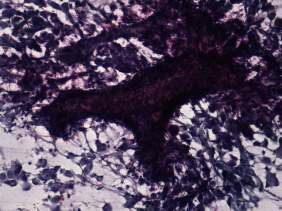
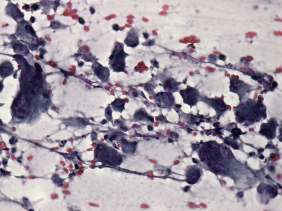
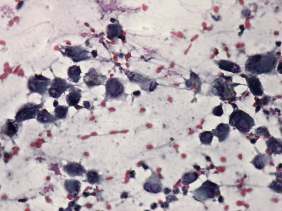
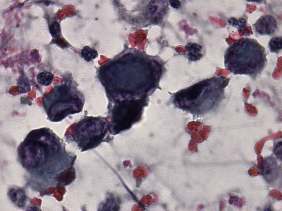
First cytological examination yielded not-diagnostic material. On a second attempt an anaplastic tumor was diagnosed with the possibility of secondary thyroid carcinoma.
Wash-out thyroglobulin resulted in 1.61 ng/mL while serum thyroglobulin resulted in 25 ng/mL. Serum calcitonin was below 0.59 pM/L.
The patient was evaluated toward a primary focus of carcinoma. CT scan, gastroscopy, colonoscopy, ultrasonography of the abdomen and pelvis were performed. Neither of these examinations revealed a tumor.
Surgical exploration was performed, and a huge tumor was found which infiltrated the trachea, the esophagus and neck muscles. Histopathology disclosed anaplastic carcinoma of the thyroid with metastases to the lymph nodes in the neck.
Comments.
-
The clinical presentation was not typical because an anaplastic carcinoma is usually more aggressive. Moreover, an anaplastic carcinoma spreads in most cases directly and lymph nodes metastasis occur not very often.
-
Until now, this was the only case in our practice in which the result of wash-out thyroglobulin determination was misleading.
-
In such large nodules which occupies an entire lobe, we lack the clue on which we can decide whether a tumor extends beyond the thyroid or not.
-
We present in the cytological pictures two very rare phenomenons, single cell necrosis and mitotic figures.
.